|
Wolfgang Michel: "Inner
Landscapes" - Japans Reception of Western Conceptions of the Body. Medicine in Japan and Germany. Japan Society for the Promotion of Science / Deutsche
Gesellschaft der JSPS-Stipendiaten. Bonn, 2000. (ISBN 3-00-005931-8) |
|
"Inner Landscapes" - Japan's Reception of Western Conceptions of the Body |
(1) Rudiments of the Japanese conception of the body
Before we turn to aspects of medicine itself, let us have a brief look at the language. Let's approach the body by means of the vocabulary the Japanese used prior to the arrival of the first Europeans. From ancient times Japanese had its own terms, of course, for head, trunk, limbs and other externally perceivable parts of the body. But as soon as we begin to delve inside the body, there's no getting round the use of Chinese terms. Heart, lung, stomach, large and small intestines, liver, spleen and many other designations testify to the heavy influence of China.
If you look through old dictionaries like the Wamyôruijûshô, a 10th-century dictionary edited according to Chinese categories, you will find among some of the entries Japanese words such as kimo for liver, yokoshi for spleen, fukufukushi for lung, murato for kidney, harawata for large intestine, hosowata for small intestine, kusowata for stomach, yubarifukuro for bladder. But with the general spread of Chinese terminology, virtually all these native Japanese terms disappeared. So it may be supposed that they were not originally part of the everyday language.[1]
Furthermore, the idea of the abdominal region (in Japanese: hara) as the seat of thought and emotion may have had old Japanese roots. Western writers like Karlfried Dürckheim pointed out this interesting notion already several decades ago (Hara, die Erdmitte des Menschen. München 1956). We encounter it not only in theories of meditation but also in many expressions still in use today, such as
hito no hara wo yomu ("read the inside of the abdomen" = read someone's mind )
kare no kuchi to hara ga chigau ("someone's mouth and abdomen are different" = he says one thing and means another)
hara wo watte hanasu ("split / open one's abdomen and talk" = be frank with a person)
hara no naka (at heart, at bottom)
hara ga kuroi ("the abdomen is black" = conceal one's real intention)
From this tradition also stems the cutting-open of the stomach, well-known in the West as hara-kiri, as an expression of the assumption of responsibility or guilt or as a final expression of protest.
In the field of medicine, this emphasis on the abdomen is most pronounced in the work of Mubun, a monk who lived in the second half of the 16th century. Rejecting the Chinese theories of "tracts and canals" - or "meridans" how some Western scholars call it - he elaborated a conception of the surface of the abdomen as a kind of representative map of the entire body for purposes of diagnosis and therapy.
(2) Views of the Body Adopted from China
Let us move on from this outline of the remnants of indigenous Japanese conceptions to the Chinese descriptions of the body that were taken up in Japan. I am going to confine my comments to what I consider the most salient points.
If you look at the writings that were adopted by Japan, you'll find that there are essentially three basic types of visual representation of the human body.
The first is a sort of flow chart of the network in the body comprising tracts and canals in which the so-called ki (Chinese qi) circulates. This ki, one of the central notions in traditional Chinese medicine and natural philosophy, bears a certain resemblance to the Greek concept of the pneuma. It pervades the microcosm of the body as well as the macrocosm of the environment in various forms and, to put it simply, keeps the life processes going. If the circulation is obstructed, in other words if there is a local excess or deficit, the upshot is illness. That is why the therapy aims chiefly at removing the excess or supplementing the shortage and ultimately restoring harmony within the body.
In Chinese as in the everyday Japanese language, a number of expressions about health, sickness, psychical condition and even atmospheric phenomena still reflect the predominance of this old conception.
But to get back to our flow chart: Representations of this type show the male body from the front, side and back. The organs are usually missing. In addition to pictures of the entire network, we also find some that demonstrate individual tracts. In many of these cases half-naked figures are depicted that remind us of monks, scholars etc. This type of representation invariably displays the human body as alive and pervaded by dynamic flows.
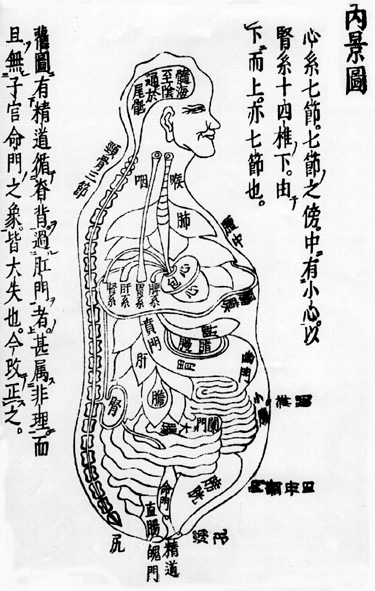
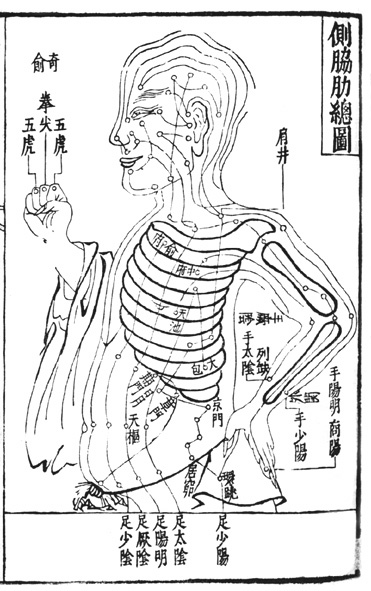
In the second type we see eleven organs that were considered important at the time. These are either depicted from the front or the side. The frontal views, which show only the organs, are fairly rare. Most of the pictures of this type give a lateral view of a limbless male body (fig.2). These illustrations, which are usually called "inner landscapes" in Chinese (and Japanese as well), are without doubt based on anatomical observations. But they have hardly changed at all since the Chinese Song era (10-13th century).
These landscapes confined themselves to the so-called "five full organs" (gozô) and "six hollow organs" (roppu) plus the spine. The body is not cut open and yet appears to be open in a strange way.
Certain characteristics of the organs shown are described in many texts, but these organs were always seen in terms of their functional relationship to the tracts and canals I mentioned earlier, and not as rigid isolated objects. So when the body was taken ill, individual organs were never taken as isolated objects of diagnosis or therapy. This also explains in part why little need was felt for precise anatomical observation and description.
These first two basic types of anatomical illustration are found in the works of the so-called "main path" of medicine (hondô), which roughly corresponds to our present-day internal medicine.
The third basic type of anatomical illustration hardly appears at all in these books. It involves the representation of "swellings" (haremono). In present-day medicine we talk about tumors, furuncles, rashes and symptomatic concomitants to a variety of diseases, but in those days there was but one single category. As maladies of the body surface, these "swellings" belonged to the domain of surgeons.
Here again, the figures portrayed were alive and sparsely clad. In all three types of illustrations that we've looked at, no muscles or shadows are shown, nor any signs of death or even dissection. Standing figures don't strike the pose that has been predominant in the West since Greek antiquity, with a standing and a trailing leg.
In the East and West, illustrations of women's bodies generally focus on their reproductive organs. Finally, the portrayals of gymnastic exercises or those of massage are not of an anatomical nature. I think the same is true of the scenes of patients and their treatment depicted in illustrated scrolls like the "Scroll of Diseases" (Yamai no sôshi). They do have a certain value for the history of medicine, but basically, like similar European works, they belong to the realm of art.
(3) The Medicine of the "Southern Barbarians" (nanban-jin) in Japan
After a brief contact in 1543, direct cultural exchange between Europe and Japan began exactly 450 years ago, in 1549, with the landing of the eminent Spanish Jesuit Francisco Xavier. In the 90 years that followed, it was chiefly Portuguese and Spanish missionaries and merchants that brought European culture to the Far East and Japanese culture to the West.
Although the Japanese called them by a less-than-flattering name "southern barbarians" (nanbanjin), they certainly respected their weapons, their skills in astronomy, navigation, surgery and art. On their imposing galleons sealed with pitch, which were dubbed "black ships" by the Japanese, the strangers brought not only European wares, but also important goods such as silk, tropical wood and medicinal drugs from all over Southeast Asia and even from Central and South America.
Actually, the Jesuits took little interest in surgical activities. For the Church had eschewed blood ever since the famous Council of Tours in the year 1163 ("Ecclesia abhorret a sanguine"). But it just so happened that Luis d'Almeida (1518-1584), a licensed surgeon who had made it rich as a merchant, joined the Society of Jesus in Japan. In Funai, Eastern Kyûshû, he founded a hospital with one hundred beds, where, as one missionary wrote, "the body was treated with medicines and the soul with prayers." In a country wracked by civil wars, there was no dearth of patients. The enthusiastic letters and annual reports from the mission testify to the popularity of the "southern barbarians' hospital".
These years are regarded as the beginning of European medicine in Japan. But the innovations were not as revolutionary as might appear. Some authors point out the new type of gunshot wound, the hitherto unknown washing of wounds with alcohol and the use of porkfat and olive oil. But injuries caused by firearms had not been known in Europe for very long either, and there was still some controversy over their nature and treatment in the 16th century. Furthermore, the missionaries were wise enough to appreciate Japanese traditions. In the hospital at Funai, the "internal medicine" was left entirely to Japanese physicians, some of whom were praised by name.
The approach to pharmaceuticals was likewise pragmatic. The bulk of the drugs came from the surrounding mountains and from Macao, Malacca and Cochinchina. Documents show that Chinese remedies and instruments were to be found in d'Almeida's dispensary. The missionaries had Chinese texts explained to them. In the mission's letters and dictionaries we find a number of indications that they delved into acupuncture and moxibustion. Luis Frois, a layman in the field of medicine, wrote that he knew how to take someone's pulse in the Japanese way. And when they fell ill, many of the European priests sought out Japanese doctors, including the famous Dôsan Manase (1507-1594) in Kyôto.
In a comparison of European and Japanese cultures in 1585, on the other hand, that same Luis Frois regretted that the Japanese would not accept urine diagnosis, phlebotomy, enema, cautery and other traditional methods highly esteemed in the West. (Schütte, 1955) Nor did Japanese field surgeons (kinsô-i) follow the example of many of their Occidental colleagues when it came to pouring boiling/hot oil into wounds.
So the interchange of medical know-how was fairly balanced and the conditions relatively favorable for a new symbiosis between the East and West. But this enterprise aborted as early as 1587 when the hospital in Funai fell victim to the strife between Japanese war lords.
From the 1580s on, the mission ran into trouble everywhere. The decades that followed until the Iberians were ultimately driven out of the country were marked by destruction, expulsion, exhaustion, illness, death. No one knows how to venesect, complained father Coelho in 1589, and three of the members of the order who fell ill from the strain of persecution have already died. When in 1591 João Rodriguez was taken ill in Kyôto, he had to travel 700 kilometers to Nagasaki for treatment. The last Christian nursing homes run by the Japanese there disappeared around 1620. To make matters worse, criticism of such medical endeavors was mounting within the Society of Jesus itself. In the end, everything relating to medicine disappeared from the writings of the Jesuits under the categorical ban ("obediencia") imposed by Francisco Pasio in 1612. Nothing remained of what had been built up under the Europeans.[2]
(4) Japanese "Southern-Barbarian-Style Medicine" (nanbanryû geka)
Today there are no known Japanese sources from which to glean how Western medicine was perceived during this second half of the 16th century. Most likely, exposure to Western concepts and methods of healing was confined to a very small group of people in a few places and during certain brief periods of time. There was no chance of any continuity due to the changeable and increasingly difficult situation of foreign and native Christians. In the wake of the destruction of d'Almeida's hospital, it is hardly conceivable that a group of Japanese doctors could have existed along the lines of Thomas Kuhn's concept of the paradigm, in other words a group that underwent similar technical training and possessed and handed down a common canon of problem-solving approaches.
And it is certainly not by chance that traces of the "southern barbarians" did not appear in Japanese medical texts until the early 17th century. The "Anthology of Everything for the Outside" (Mangai shûyô), which dates from 1619, is considered the oldest work of "southern barbarian style medicine". But the mention of five plasters, washing wounds with spirits, and some instruments like scissors and scalpel goes to show that, even after seven decades of East-West contact, there were still some writers who knew almost nothing about Western surgery.
Standard Japanese works on the history of medicine name Dôki Kurisaki (1582-1665) as an exponent of "surgery in the style of the southern barbarians" (nanbanryû geka). He is said to have gone to the Philippines as a child and undergone training there. From 1617 on he worked as a physician in Nagasaki, where some Portuguese were still living until 1638 and where two years later the Dutch East India Company was to set up a trading post.
The teachings compiled by his pupils, however, reveal a blend of Japanese, Chinese, Iberian and Dutch elements. If he really received training in Western methods, one ought to find more European elements. What's missing is anatomy, for instance, to which great importance was attached at European universities as well as in the surgeons' guilds. The presentation of furuncles, a focal point of Kurisaki's teachings, shows no trace of the systematic arrangement you find in Western works on the subject. Either Kurisaki's pupils only set down what they understood, or he had merely acquired some practical skills and rudimentary knowledge in the Philippines. Anyway, though he clearly became a successful phsycian in Nagasaki, he can hardly be regarded as a representative figure of "southern-barbarian-style surgery."
It is not impossible that some new material will be found, however, it is not purely by chance that to this day not a single reference to any Western work on medicine, surgery, anatomy, pharmacy is known in any manuscript dating from the long period between the advent of the Iberians' in 1549 and their final expulsion in 1638.
And that is in spite of the fact that the language barriers were not all that high then, certainly much lower than in the following two centuries. Some of the Europeans spoke excellent Japanese and many Japanese spoke Portuguese just as well, some even Latin.
|
Period of "Isolation" |
|
|
1401 - Early Chinese Wave II |
Late Chinese Wave II |
|
1543 - Iberian Wave - 1639 |
1641 - Dutch Wave - 1854 |
What's more, the social and intellectual conditions were quite favorable for the reception of new knowledge and thought. For one thing, many scholars parted with Buddhism. For another, the efforts of the regional rulers to bolster their domains through overseas trade with East and Southeast Asia led to the adoption of a number of foreign innovations, many of which stemmed from China (cf. fig.3). To name just a few: improvements in smelting and forging methods, in papermaking, silk-weaving, book-printing, and some in ship-building and navigation as well. Most of this know-how was disseminated not by Buddhist monks or scholars as in the past, but by merchants and artisans; hence it was predominantly of a practical nature.
Consequently it was not due to a lack of intellectual receptiveness that the Iberians' medicine did not take root firmly in Japan. Given the destruction of the mission hospital in Funai, the mounting persecution of Christians and also resistance within the Society of Jesus, there was no stable basis anymore for an effective interchange. So, to take issue with the standard literature on the subject to date, I do not believe the Japanese ever came to practice "southern-barbarian-style surgery" in the sense of a paradigm that could be passed on or handed down to succeeding generations.[3]
(5) Another Try
The Dutch reached Japan at the beginning of the 17th century. Probably because most of them had blonde hair, partly with a reddish tinge, they were dubbed redheads (komôjin) by the local people. In 1609 they established a trading post on the western Japanese island of Hirado. Then in 1641 they were forced to move to the small manmade island of Deshima (Dejima) in the Bay of Nagasaki.
Thanks to their lack of interest in proselytizing and their tactical acumen, they were the only European nation left that was permitted to land at Japan. Until Japan's reopening-up to the West in the mid-19th century, the entire exchange of goods and information between Europe and Japan took place via this little trading post of about 200 by 65 meters size.
In the mid-17th century, interest in the Western art of healing arose anew in Edo and Nagasaki. In the history of Japanese medicine the name of a German surgeon, Caspar Schamberger, is associated with the birth of the so-called "Caspar-style surgery" (kasuparu-ryû geka). Probably without even suspecting it, he sparked a lasting interest in Western medicine, herbal lore and pharmacology. Under the influence of Schamberger's successors at the trading post on Dejima, other surgical approaches followed and combined with other disciplines to form "Dutch studies" (rangaku), as it was called, which was to lay the foundation for the rapid modernization of the country beginning in the second half of the 19th century.[4]
Here, as elsewhere, historical processes are seen to be influenced by a wide array of factors. For example, chance played a part when the shôgun Ietsuna Tokugawa was taken seriously ill in 1650 and the Dutch legation that had come to Edo had to wait for months for an audience. Suffering from diseases of old age, some high-level officials sought out the foreign surgeon Schamberger, which served to give prominence to the apparently effective medicine of the "redheads."
And then there were structural factors. By confining their external relations to only a few partners, those in power became acutely aware of their dependence on certain goods and know-how. The adoption of certain Western know-how proved beneficial not only to their own health, but also to the further development of the country and thus the consolidation of power. In addition to medicine, weapons, astronomy and cartography were of special interest. These developments were largely due to the far-sightedness and influence of particular individuals. For example, the dynamics of these decades cannot be adequately explained without taking into account the influence of the imperial inspector general Masashige Inoue.
Although this new knowledge was handed down only from teacher to pupil, from father to son, it soon spread throughout Japan. The first printed books appeared only two decades after Schamberger (Oranda geka ryôhô,1661; Kômô hiden geka ryôjishû, 1684). Regional lords sent their personal physicians to the Dejima trading post surgeons. Books, drugs, herbs and medical instruments were ordered at high prices. Despite on an import ban for Western books many works on medicine, pharmacy and natural sciences entered the country throughout the 17th century. It should be pointed out that it was always the Japanese who took the initiative, requested information, placed orders, selected, took up or rejected what the rather reluctant Europeans had to offer. In view of this boom, it's surprising that the developments that characterized the 19th century did not materialize already in the 17th century. But closer scrutiny shows that the Japanese still had a number of reservations about Western medicine and that a new barrier had appeared.[5]
(6) The Limits of "Redhead-Style Surgery"
The Japanese "surgery in the style of the redheads" did not go beyond the confines of European "low-level" or "minor surgery". This isn't surprising in view of the professional training of the East India Company surgeons, though even in this small field of endeavor the Japanese confined themselves to specific tasks.
The same subjects are dealt with again and again in the manuscripts and copies of manuscripts from that epoch: plasters, ointments and the treatment of wounds and fractures. You will search in vain for any references to cataract operations, cystolithotomy of bladder stones, bone trepanning, or amputations - operations that were indispensable for any ambitious surgeon in the Occident. Cauterization and phlebotomy, which was still practiced in the West in the early 19th century, were abhorred by the Japanese. And not a word about human anatomy, which was considered fundamental not only at European universities but also in the training of apprentices by the guilds. Indeed, you won't find more than a few names of bones and a couple paltry remarks on "arteries," "veins," on a "thin skin around the brain" and the "skin between the chest and abdomen."
Euro-Japanese communication had deteriorated dramatically since the days of the Christian mission. It was considered undesirable that the Dutch acquired a knowledge of Japanese language. But up to the end of the 17th century the language skills of the Japanese interpreters only sufficed for business negotiations and everyday conversation, not for reading scientific books. So people had to have everything explained and demonstrated to them by the trading post surgeons. As is shown by the official diaries of the trading post, such instructions were a night-mare for everyone involved.
Since the Japanese couldn't understand many of the Latin and Portuguese medical terms, they just noted the pronunciation in Katakana syllabary. The meanings of the names of medicines, herbs and so forth were found out by and by.
On the subject of humoral theory, in contrast, a single brief abstract was drawn up in the 17th century, which was probably not understood by any Japanese readers. The philosophical and scientific bases of Western medicine remained inaccessible; nor was any notice taken even of the dynamic advance of medicine in Europe. Ultimately, the reception did not go beyond specific projects. And that was not enough by any means to cut out Sino-Japanese medicine.[6]
Educated Japanese could read the literature from China. And since Japanese thought had evolved over the course of centuries through an ongoing interaction with China, Chinese ideas could be more readily assimilated. It was precisely in the 17th century, moreover, that Chinese science and Confucianism were understood and embraced as comprehensive systems - maybe for the first time ever in Sino-Japanese intercourse. To consolidate its own power, the new Tokugawa regime actively promoted the adoption of Confucianism as interpreted by the 12th century Chinese scholar Zhuzi oder Zhuxi (Japanese Shushi), a version with a strong emphasis on submission to authority. Thanks to the establishment and expansion of libraries and a number of private and feudal clan schools, there emerged a kind of academic infrastructure. This served to enhance the prestige of Chinese medicine, particularly as many Confucian scholars earned their living as physicians.[7]
Those open to Western therapies also took this Sino-Japanese medicine as a theoretical basis. But, as already mentioned earlier, this approach attached great importance to cosmic harmony and freedom from bodily harm. That left only little room for "invasive" surgical measures. Presumably Japanese doctors in the 17th century did have enough opportunity to see the organs and so forth of the seriously injured. Surely they knew there were many things in there, maybe they even took a closer look at them. But at the end of the day, the form, color, composition and position of the stomach, liver or heart meant nothing to them.
Small wonder, therefore, that they didn't take all that much interest in the European surgeons' explanations of human anatomy. For Japanese physicians, these explanations did not figure prominently either in theory nor in their day-to-day practice of medicine. In the second half of the century, an interpreter by the name of Shôdayu Motoki (1624-1697) drew pictures from a book entitled Pinax Microcosmographicus by Johannes Remmelin and provided a simple summary in Japanese. Some physicians, like Sanshin Hara in Fukuoka, even took the pains to make themselves a copy of it.[8] Nevertheless, this work had no impact at all during that period.
(7) The First Post-Mortem
We are now going to take a leap into the 18th century. It took about one hundred years before a Japanese doctor opened up a human cadaver [kadei] to take a closer look at the "inner landscapes".
Interestingly enough, this Tôyô Yamawaki (1705-62), nowadays extolled as a pioneer, was not a proponent of Western surgery, but of the so-called "Ancient Practice School" (ko-ihô-ha). Under the influence of thinkers like Jinsai Itô (1627-1705) and Sorai Ôgyû (1666-1728), these physicians had liberated themselves from the doctrines of Zhuxi, the Chinese Confucianist I mentioned a little earlier. Zhuxi's system, which comprehended nature, man and society, formed an ideological pillar of the Tokugawa regime. His teaching, however, was of a theoretical nature and full of speculative elements, so it was often hard to apply to real-life problems. This is why it had been criticized by Japanese scholars ever since the 1660s.
However, the physicians of the "Ancient Practice" (based on the ideas of Itô and Ôgyu) were by no means out to modernize science, but more engaged in a kind of revisionism. They had come to appreciate the importance of observation and experience through the study of a Chinese book entitled "Treatise on Febrile Diseases" (Shanghan lun, Japanese Shôkan-ron) written by Zhongjing Zhang in about 200 ad. At first, their interest focused on the symptoms of diseases and the effects of medicaments. But gradually they also turned to a field that would later pave the way for the success of Western medicine in Japan: anatomy.
As early as 1722 Noritada Hattori had raised the question of "how a doctor can keep someone alive without any knowledge of internal organs." In his "Illustrated Explanation of the Inner Landscape" (Naikei Zusetsu, 1722) he presents a new system he had designed, in addition to the traditional Chinese picture of the "five hollow organs" and "six full organs" (gozô roppu). This was the first work to criticize the traditional representation of the organs.
A certain influence may be attributed to Tôshuku Negoro's systematic studies of the skeleton, performed on decomposed bodies of two criminals who had been executed. The results were published in 1741 in the "Atlas of the Human Skeleton" (Jinshin renkotsu shinkei-zu).[9]
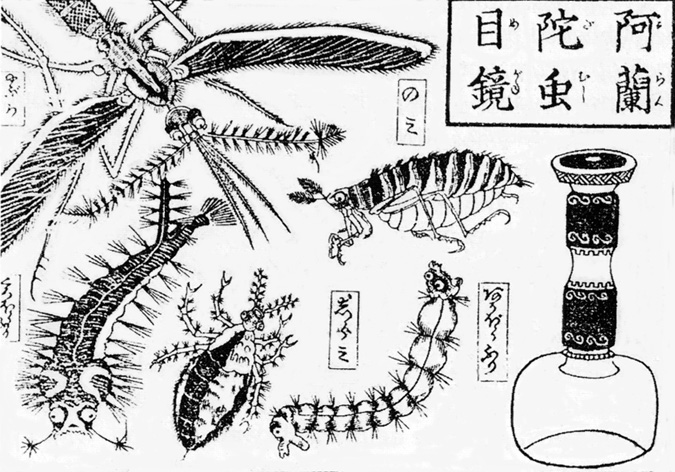
And at this point, we should also take a glance at some other influences from the West. In the second half of the 17th century and more so in the 18th century, Japan imported mirrors, spectacles, magnifying glasses, microscopes (fig. 4), telescopes and zograscopes.[10]
These articles had a substantial impact on the way things were seen, which was increasingly reflected both in language and in art and had its influence on scholars too.
(8) Tôyô Yamawaki's search for the 'Nine Organs'
As I already mentioned the first major stride forward was taken by Tôyô Yamawaki (1705-62), a member of the "Ancient Practice School" (ko-ihô-ha). The dissection of human bodies was forbidden since it conflicted with the tenets of Buddhism. However, Yamawaki and Genteki Kosugi (1734-91) managed to obtain permission from the authorities to perform a dissection. In 1754 they had the body of an executed criminal opened up in Kyôto. Five years later Yamawaki published the results of this dissection under the title "Record of the Viscera" (Zôshi). The woodblock illustrations were made by Sukemitsu Asanuma.
Yamawaki's teacher, the famous scholar Gonzan Gotô (1659-1733), had once suggested he dissect an otter. When Yamawaki did so, he could only find eight of the "nine organs" mentioned in the old Chinese classic "Rites of the Zhou" (Zhouli). What he did then was typical. He went to his bookshelves and studied other very old Chinese writings like Shujing ("Book of Documents"), Liezi ("Book of Master Lie"), Guoyu ("Sayings of the States"). But they differed widely on the number of organs. Only then did it occur to him to open up a human body and find out for himself.
It is doubtful whether this account by Yamawaki sufficiently explains his motivations for performing a dissection. But one thing is clear: the dissection enabled him to confirm the nine-organ theory and, in consequence, the authority of the classic "Rites of the Zhou". Yamawaki really wasn't looking to break now ground, he wanted to "get back to the future". His view of the body was wholly informed by tradition. Characteristically enough, he had the dissection performed by a butcher - in other words, a member of an ostracized group. The crudeness of the illustrations in his book cannot be attributed merely to the limited nature of the research objectives or the lack of the draftman's artistic ability. Like his later successors, Yamawaki had to conclude the dissection within a single day.[11]
Most likely, Yamawaki had hardly foreseen the consequences of his investigation. The attacks were vehement and came in part even from the "Ancient Practice School" itself. Its pioneer, Tôdô Yoshimasu (1702-1773), for example, considered the clinical description of diseases and therapy more important than any contemplation of theoretical bases. In his "Medical Talks" (Idan), published in 1759, he wrote that knowledge of anatomy was superfluous in treating the sick. That wasn't entirely untrue. For insights of that kind could not be used in practice. An even more aggressive reaction came from Yasudo Sano in his "Anti-Viscera-Book" (Hi-Zôshi, 1760). In his opinion, the most important thing about an organ isn't its shape, but its spirits, its vitality (shin, ki ). Once they're gone, the organ is but an empty shell. This view has its modern implication by making the dead body just a lump of flesh.[12]

The approving reactions, too, led in a different direction to what Yamawaki had supposed. Even before his book was printed, more post-mortems were carried out, and the classical nine-organ theory that he had apparently corroborated was soon refuted by new observations.[13]
Without doubt, Yamawaki's post-mortem examination was revolutionary by Japanese standards at the time. A commemorative stone has now been placed at that very spot in Kyôto, and I think that's justified. Nonetheless, I don't think his work was yet the dawn of modern medicine. Yamawaki was not a discoverer like the Renaissance anatomist Vesalius, for instance. To be frank, his approach reminds me more of the dissections performed in Europe in the Middle Ages.
In the 13th century, professors at the university of Padua and elsewhere read aloud from the works of grandsire Galen. Down at the table stood a surgeon, cut open the cadaver and exhibited the parts that were just being discussed: the quintilobular liver and other peculiarities of Galen's anatomical teaching. Here, as in Yamawaki's endeavors, the object was to confirm the authority, not to demolish the tradition and discover new things.
As in ancient Egypt and Peru, "seeing" does not mean "observing" in Yamawaki's investigations. Needless to say, Japanese doctors had been seeing the insides of dead bodies for many centuries: on the battlefields, at the sites of accidents and other incidents. The razor-sharp swords of Japanese warriors split their enemies' bodies every which way like soft sausages. Yet the form, color, consistency of the things the doctors beheld there were of no great importance to them. They only perceived what they knew.
Thus, to my mind, Yamawaki's historical accomplishment lies not in the nature and results of his dissection, but in the sheer fact that he carried out a dissection. For that established a precedent others could cite when requesting permission for a dissection.
(9) Genpaku Sugita and the "New Book on the Dissection of the Body"
In the history of Japanese medicine, the translation of Johan Adam Kulmus' "Anatomische Tafeln" (Anatomical Plates, 1722) into Japanese is usually celebrated as the next great pioneering feat. You won't find an educated Japanese person who doesn't know the names of the translators: Genpaku Sugita (1733-1817) and Ryôtaku Maeno (1723-1803). The two of them had an opportunity to watch a dissection in 1771. Comparing what they saw to the illustrations in Kulmus' book, they found that the latter were quite exact. On the way home they decided there and then to translate the book.
But at that time, their language skills were wholly inadequate to the task. In his "Memoirs on the Beginning of Dutch Learning" (Rangaku koto hajime, 1815), which he wrote decades later, Sugita himself gives a touching account of their agonizing struggle with a virtually unknown language: how - in his words - they crossed a stormy ocean in a rudderless ship.
Their translation came out in 1774 with the title "New Book on the Dissection of the Body" (Kaitai shinsho). The book was a tremendous success. Not only did it show one way of obtaining new knowledge from Europe. Thanks to Sugita, the realization spread that the observation of singular phenomena should be combined with the search for the underlying fundamental principles (Sorai Ôgyû). In other words, that knowledge of human anatomy eventually would improve the practice of medicine.[14]
(10) Shinnin Kawaguchi (1736-1806)
I certainly do not want to depreciate the historical achievements of Sugita and Maeno, but I would like to take this opportunity to present a physician who accomplished a similarly significant and pioneering feat even before these two, but who has long been paid too little homage in the history of Japanese medicine.
As a young man, Shinnin Kawaguchi studied first with Dôi Kurisaki, an exponent of the Western-oriented surgery, as well as with the famous phsician and interpreter at the Dutch trading post, Kôgyû Yoshio (1724-1800). During those years in Nagasaki, he copied and received a great deal of material, including the Syntagma Anatomia, the famous work on anatomy by Johannes Vesling.
As physician to the House of Doi, he went to Kyôto in 1769 when Lord Toshisato Doi was appointed "Kyôto Deputy" (Kyôto shoshidai) of the Tokugawa government. At that time Yamawaki had already been dead for seven years. In Kyôto, Kawaguchi became a pupil of the renowned physician Gengai Ogino (1737-1806). Permission for a dissection had to be requested from the Kyôto Deputy, which made things easier for Kawaguchi, being the Deputy's personal physician. In 1770 he was allotted two cadavers and a head at the place of execution in Kyôto. That was the fifth dissection to be done in Japan. [15]

Unlike Yamawaki and Kosugi, Kawaguchi does the carving himself - with one straight knife and one curved one. As you can see, these were pretty crude instruments. With a vigorous incision the 35-year-old physician slashes open the thorax from the throat to the solar plexus. Before him the heart and lungs lie exposed. After having determined their positions, he resects the organs. He notes their size, color and consistency. Beside him is Iki Harada, likewise trained in Nagasaki, who has been waiting a long time for an opportunity like this. Harada takes the organs that are passed to him and subjects them to further scrutiny. He inflates the lungs with a bamboo pipe, then inspects the intestines inch by inch to see how the contents change. Their teacher, Ogino, is sitting nearby, naming the organs and commenting based on his previous experience in the dissection of otters. Another seven pupils are in attendance.[16]
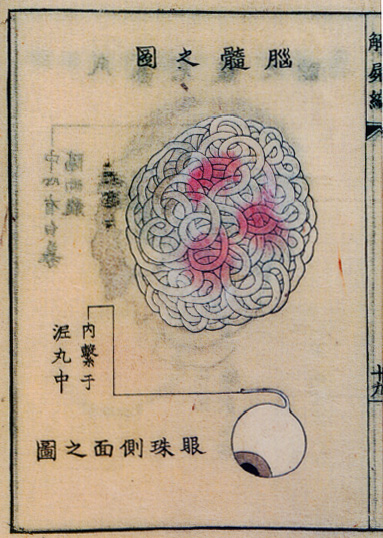
Kawaguchi and Harada's attitude towards the cadaver differs greatly from that of Yamawaki. There's no searching through the classical literature anymore, no more hesitation, no detached reflection and no awe from the knife and body fluids. Nor do they feel the need to compare their observations with illustrations in Western books. This is a cold, modern-looking search for new insights. Kawaguchi is the first man in Japan to dissect the brain, which did not figure very prominently in traditional medicine. And he goes after the eyes (fig.8).
Kawaguchi's teacher was opposed to publishing the notes. He didn't want the famous Yamawaki to be contradicted. He was also afraid their findings, which could not be made use of in practice yet, would rock the very foundations of traditional medicine and jeopardize medical care throughout the country as a result. But his opposition was in vain. These were no longer the physicians of the 17th century, who only passed their knowledge on to their pupils. Kawaguchi had the woodcuts executed for him by Shunmei Aoki and proceeded to have his "Notes on Autopsy" (Kaishihen) published in 1772. After Yamawaki's "Record of the Viscera" (Zôshi), his was the second book of its kind in Japan.[17])
What made it possible for these books to have a widespread impact was at least in part the open-mindedness of the new Senior Imperial Councilor, Okitsugu Tanuma (1719-88). Tanuma had worked his way up to this powerful position from the lowest ranks, and he strove resolutely to further develop the economy and trade. Apparently, this dynamic and pragmatic man was well disposed towards the publications. When neither Yamawaki nor Kawaguchi and Sugita had met with a hostile reaction from the authorities, there was no more hesitation. Dissections ensued almost all over the country, accompanied by flood of publications and intensive studies of Western writings in other fields too, which we refer to by the catchword "Dutch Learning" (rangaku).
(11) 18th-Century Japanese Illustrations of Dissections
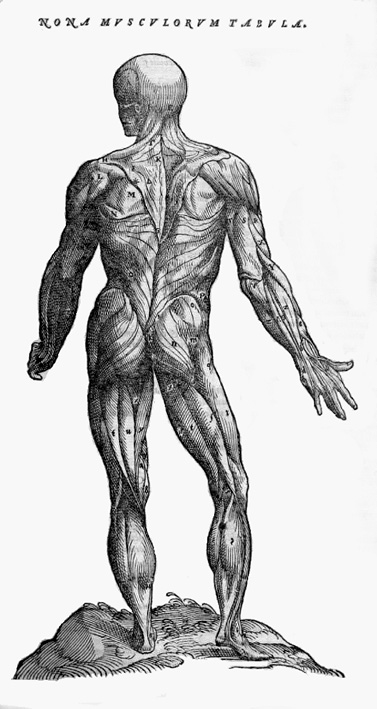
In closing, allow me to make a few remarks about Japanese anatomical illustrations of the 18th century. From the days of Vesalius, European illustrators had endeavored to assuage the viewer's fears by presenting the corpse as more or less alive. It was idealized in its proportions and often portrayed in the poses of Greek antiquity.(Roberts / Tomlinson, 1992) Though their bodies have been opened up, these figures feel no pain, nor are any body fluids flowing.
The Japanese artists and physicians of the 18th century had a completely different pictorial language. They showed a cadaver, usually with recognizably individual traits. Many of these bodies even bear their own names or a kind of nickname: Heijirô, Aocha-baba ("old auntie Aocha") etc. Furthermore, all the manuscripts and prints of that epoch are colored in. In many cases, blood and other body fluids are flowing, the odor of death is spreading and makes the viewer uneasy.
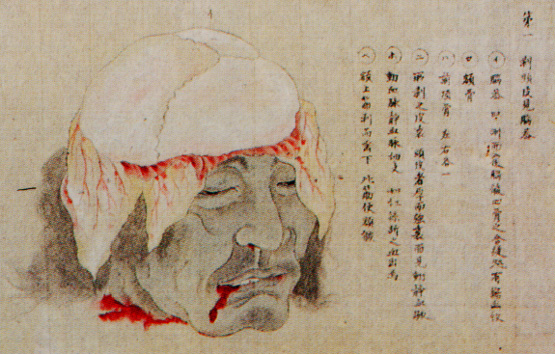
The scientific value is problably less than that of comparable old Western illustrations. But in a certain sense they are more realistic. That's because they depict not so much the results of a dissection as the dissection process itself.
In hand-painted picture scrolls we even find stories that go from the execution to the preparatory arrangements for the post-mortem and on to the complete dissection of the cadaver.

These images indicate the degree to which those involved were already capable of looking straight at the exposed viscera.

Final Remarks
The road was now paved for a new conception of the body. The subsequent strides were remarkable. Body and soul were separated, at least as far as possible. Diagnosis and therapy were no longer aimed exclusively at the patient as a whole, but from case to case at specific organs, specific spots in the body. The canonization of the old texts was abandoned, theory and practice were dynamized. 19th-century dolls and popular prints that reveal the secrets of the human body in a mechanical and functional manner testify to the rapid spread of this novel way of seeing things among the general public as well.
This departure was at once an expression of and a stimulus to socio-political change. In the Edo period the foundations were laid for the unprecedented modernization of the country that followed the opening-up of Japan in the mid-19th century. The pioneers who painstakingly groped their way forward in a difficult state of isolation deserve all our respect, in medicine as in any other field.
1955 Schütte: Josef Franz (ed.): Luis Frois, Kulturgegensätze Europa-Japan (1585). Sophia Universität, Tôkyô 1955.
1978 Sakai, Shizu / Ogawa Teizô: 'Kaitai shinsho' shuppan izen no seiyô igaku no juyô. In: Nihon gakushi-in kiyô, Vol. 35 (1978), No. 3, 129-151.
1982 Achiwa, Gorô: Kindai Nihon no igaku - Seiyô igaku no juyô to kiseki. Shibunkaku shuppan, Kyôto 1982).
1989 Rosner, Erhard: Medizingeschichte Japans. Brill, Leiden / New York / København / Köln 1989.
1989 Sugimoto, Masayoshi / David L. Swain: Science & Culture in Traditional Japan. Tuttle, Tôkyô 1989.
1989 Sôda, Hajime: Nihon iryôbunka-shi. Shibunkaku shuppan, Kyôto 1989.
1991 Nagayo, Takeo: History of Japanese Medicine in the Edo Era. University of Nagoya Press, Nagoya 1991.
1992 Roberts, K.B. / Tomlinson, J.D.W.: The Fabric of the Body. European Traditions of Anatomical Illustration. Clarendon Press, Oxford 1992.
1993 Michel, Wolfgang: Frühe westliche Beobachtungen zur Moxibustion und Akupunktur. In: Sudhoffs Archiv für die Geschichte der Medizin., Bd.77, Heft 2 (1993), S.193-222.
1995 Hara, Sanshin (ed.): Nihon de hajimete honyaku shita kaibôsho. Rokudai Hara Sanshin ranpô-i 300nen kinen shôgakkai, Fukuoka 1995.
1996 Screech, Timon: Western Scientific Gaze and Popular Imagery in Later Edo Japan. Cambridge UP, 1996.
1996 Uchiyama, Junichi: Edo no kôkishin. Kôdansha, Tôkyô 1996).
1996 Yôrô, Takeshi: Nihonjin no shintai-kan no rekishi. Hôzôkan, Tôkyô 1996.
1997 Michel, Wolfgang: Kômôryû geka no tanjô ni tsuite. In: Yamada / Kuriyama (1997), pp.231-263.
1997 Sakai, Shizu: 18-seiki no nihonjin no shintai-kan. In: Yamada / Kuriyama (1997), pp.431-455.
1997 Sugitatsu, Yoshikazu: Edo-jidai kaibô no jiseki to sono hankyô. In: Yamada / Kuriyama (1997), pp.503-542.
1997 Unschuld, Paul U.: Chinesische Medizin. C.H. Beck. München 1997.
1997 Yamada, Keiji / Kuriyama, Shigehisa: Rekishi no naka no yamai to igaku. Shibunkaku shuppan, Kyôto 1997.
1997 Yamada, Keiji: Yamawaki Tôyô no kaibôgaku to shokugyô oyobi gakumon toshite no i no jiritsu. In: Yamada / Kuriyama (1997), pp.457-487.
1998 Kawashima, Junji: Doi-han rekidai ran'i Kawaguchi-ke to Kawaguchi Shinnin. Kindai bungeisha, Tôkyô 1989.
1998 Koga rekishi-hakubutsukan (ed.): Nihon kaibô koto hajime - Koga han'i Kawaguchi Shinnin to sono keifu. Koga 1998).
1999 Michel, Wolfgang: Von Leipzig nach Japan. Der Chirurg und Handelmann Caspar Schamberger (1623-1706). Iudicium, München 1999.
